


THE MAN WHO BECAME HUMANITY (WITHOUT ASKING) AND THE FIFTY YEARS OF DETRIMENTAL CONSEQUENCES FOR WOMEN.
- THE EVE DIRECTIVE H.Q

- 7 days ago
- 10 min read
// BLUNTBIRDS REPORT //
Reported by // Special Agents // Georgie F. & Aubrey R.
Unit // BluntBirds // Intelligence Division
Classification // [H.Q.] Approved for Public Access
// TRANSMISSION START //
⚠️ CRITICAL INTEL DISCLAIMER ⚠️
This report documents the formal regulatory architecture that established a single male body type as the universal human standard across medicine, engineering, vehicle safety, and building design and examines what that produced across fifty years of downstream consequence. All claims are sourced from peer-reviewed research, verified institutional data, and documented public record.
Contents classified as: REBELLIOUSLY ACCURATE.
// INVESTIGATIVE BRIEF: WHAT THIS REPORT UNCOVERS //
For decades, modern global systems were quietly built around a single biological default: the Reference Man — a 70kg Caucasian male standard formalised in 1974 for scientific modelling. That benchmark spread far beyond radiation research into medicine, crash safety, workplace design, drug testing, and diagnostic frameworks still used today across Australia, the United States, and the United Kingdom*.
This report investigates how male-default research shaped modern healthcare and engineering systems — and examines the structural consequences of designing “universal” architecture around a body that was never actually universal.
Key Pillars of This Investigation:
The Clinical Data Deficit: How the FDA’s formal exclusion of women from clinical trials (1977–1993)* created a 50-year drug dosage gender gap* and systemic cardiovascular misdiagnoses*.
The Neurodivergent Diagnosis Gap: Why adult women face an average 5-year delay for ADHD and autism diagnoses* due to diagnostic criteria and assessment tools calibrated almost exclusively on male presentation.
The Architecture of Discomfort: How global building climate systems (ASHRAE Standard 55)* overestimate female resting metabolic rates by 19% to 35%*, turning the standard office thermostat into a documented drag on female workplace productivity.
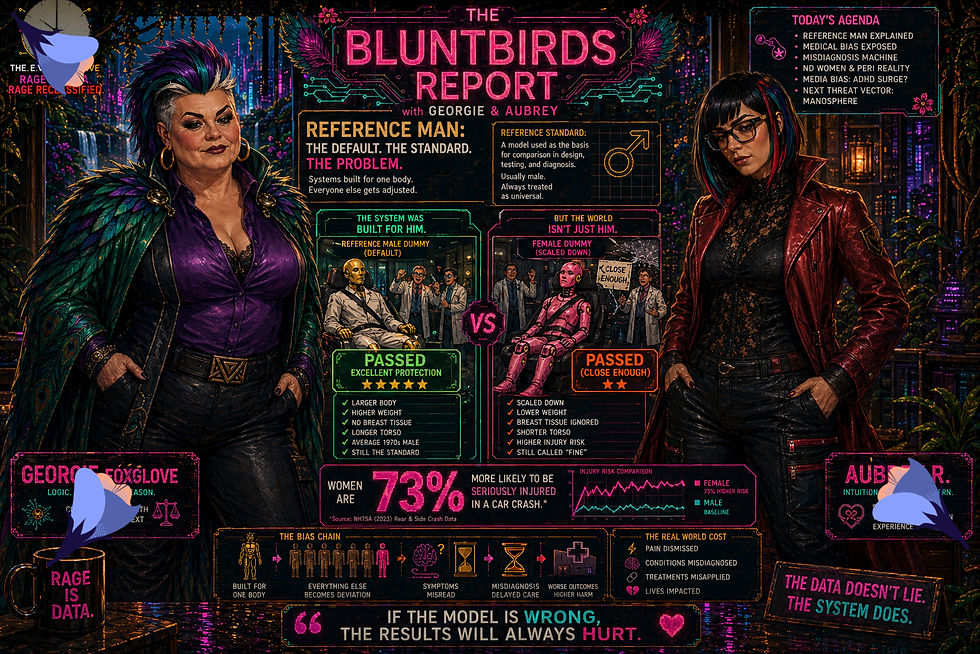
The Vehicular Safety Disparity: Why women are 73% more likely to be seriously injured in equivalent frontal car crashes* because crash-test dummies weren't modeled on average female biomechanics until 2022*.
Using peer-reviewed research, institutional data, and documented public records, this investigation isolates the hidden historical architecture that turned one theoretical body into everyone's problem.
// FIELD TRANSMISSION //
// SUBJECT: The Unmistakable Pattern and the Man Behind It //
Monique* is forty two years old, sitting in a GP's waiting room in suburban Melbourne on a Tuesday morning, holding a handwritten list of symptoms she compiled over six months. The list, she learned after several appointments that went nowhere, was necessary — arriving without documentation tends to produce a prescription for something she does not need. The symptoms include joint pain that woke her at 3am for eleven consecutive nights, a cognitive fog severe enough that she missed a deadline she had not missed in twelve years, heart palpitations attributed at a previous appointment to anxiety, and an emerging intolerance to a medication she had taken without incident for four years.
What she does not know, sitting there, is that the dosing guidelines for that medication were established in clinical trials conducted predominantly on male subjects. What she cannot yet name — because the architecture that produced her situation was never made visible, is that the problem is structural, historical, and part of a much larger pattern.
This pattern in particular even has an official name. It is called the Reference Man.
THE DOCUMENT THAT BUILT THE DEFAULT
In 1974, the International Commission on Radiological Protection published what was intended as a narrow administrative tool. It needed a physiological baseline for calculating radiation dosimetry and occupational safety thresholds — a theoretical human whose body dimensions, organ weights, and metabolic parameters could anchor research and regulatory calculations. The commission described its reference subject as a Caucasian male, aged twenty to thirty, weighing seventy kilograms, approximately one hundred and seventy to one hundred and eighty centimetres tall, with a standard body surface area of 1.8 square metres. He was named the "Reference Man." We like to call him "Gerald."

He was not designed to govern pharmaceutical dosing, diagnostic criteria, vehicle safety protocols, or building climate systems. The commission's remit was radiological protection, and the Reference Man was its arithmetic convenience. What happened next is the story of how institutional logic migrates across domains without examination.
His physiological assumptions were subsequently inherited across adjacent systems such as HVAC engineering standards, crash test protocols, drug dosing tables, and the diagnostic frameworks used by clinicians across Australia, the United States, and the United Kingdom today because institutions, when they need a baseline, tend to reach for the one that already exists. The question of whether that baseline was representative was not asked with much urgency for decades. By the time it was asked consistently, the infrastructure built around the answer was deeply embedded.
THE BUILDING RECORD: WHEN THE THERMOSTAT BECOMES A PRODUCTIVITY INSTRUMENT
The Predicted Mean Vote thermal comfort model — developed by engineer P.O. Fanger in the late 1960s and currently embedded in ASHRAE Standard 55, the building standard governing indoor climate for billions of people globally — calculates office heat load using a metabolic rate derived from male biological baselines. The standard assumes every occupant radiates approximately 120 watts. In 2015, Boris Kingma and Wouter van Marken Lichtenbelt published research in *Nature Climate Change* demonstrating that this standard overestimates female resting metabolic rate by between nineteen and thirty-five percent.
The result, played out across the HVAC systems of most commercial buildings globally, is a chronic pattern of mechanical overcooling with documented demographic consequences. A 2021 study published in Scientific Reports by Parkinson, Schiavon, de Dear, and Brager — drawing on 38,851 occupant surveys across 435 US office buildings in 168 cities — found that women are 1.8 times more likely to experience thermal dissatisfaction than their male colleagues. During summer months, seventy-six percent of cold-office complaints originated from women.

Rather than revising the underlying metabolic baseline, ASHRAE guidance continued to rely substantially on clothing-adjustment assumptions — the position that thermal discomfort in women reflects differences in what they wear rather than how the model was calibrated. The international building standard was updated in 2023. Its metabolic rate tables retained the male baseline. A 2025 meta-analysis by Vellei, Pallubinsky, Khovalyg, Carter, and Chinazzo, published in *Building and Environment*, confirmed that the PMV model fails to accurately predict female thermal sensation votes, it correlates with male experience and diverges progressively as temperatures drop.
The economic dimension of this failure has been quantified. Research published in PLOS ONE in 2019 by Chang and Kajackaite found that for every one-degree Celsius increase in ambient temperature, female performance on mathematical tasks improved by 1.76 percent — a finding of high statistical significance. Male performance declined by 0.63 percent, a change that did not reach significance. The cold office is not a comfort complaint. It functions as a productivity instrument, and its calibration is not neutral.
THE VEHICLE RECORD: 136 YEARS, AND THEN A DUMMY
The automobile was invented in 1886. In 2022, Dr. Astrid Linder at the Swedish National Road and Transport Research Institute introduced the first crash-test dummy specifically engineered around average female biomechanics rather than scaled male proportions. The 136-year gap between those two facts is not an oversight. It reflects a consistent pattern in which the bodies most frequently occupying vehicles were not the bodies around which vehicle safety systems were designed.
The female crash test proxy that preceded Linder's work was not derived from female biomechanical data. It was a scaled-down male model — typically representing a smaller male, meaning female injury risk patterns were being approximated rather than measured. A 2019 analysis from the University of Virginia found that women wearing standard seatbelts are seventy-three percent more likely to sustain serious injury than men in equivalent frontal collisions. Fatality risk runs between seventeen and twenty percent higher for female occupants, with updated confirmation from the Medical College of Wisconsin in 2024.
When this data emerged in research literature, explanatory frameworks frequently emphasised behavioural factors — driving position, seat adjustment, vehicle choice. The design parameters of the safety systems themselves attracted less institutional attention. The seatbelt was engineered to engage the geometry of male hip bones. Airbag deployment thresholds were calibrated for an unbelted adult male in a high-speed frontal collision; between 1996 and 2000, the NHTSA documented 179 people including 118 children killed by airbag deployment in low-speed crashes that should not have been fatal. The system functioned as designed. It was designed for a different body.
// FUCKED FACTS WITH GEORGIE //

Apple's HealthKit platform launched in 2014 tracking seventy-six health metrics: blood alcohol content, molybdenum intake, daily sodium, respiratory rate. It could not track a menstrual cycle. Period tracking was added the following year, under public pressure. Critics noted that the omission reflected broader patterns in male-dominated technology design — the engineering workforce at the time was approximately seventy percent male.
A 2020 analysis by Zucker and Prendergast, published in Biology of Sex Differences, identified a drug dosage gender gap across eighty-six FDA-approved medications — including antidepressants, cardiovascular drugs, and analgesics. Because dosing parameters were established in trials conducted predominantly on male subjects, women experience disproportionately high rates of adverse drug reactions linked in part to dosage standards historically calibrated on predominantly male trial populations. The dosing guidelines remain in clinical use.
The standard piano keyboard was calibrated to a key width optimised for average male hand span. Research consistently shows that a seven-eighths keyboard substantially reduces ergonomic disadvantage and injury risk for many players with smaller hand spans. Adoption by the industry remains minimal.
THE MEDICAL RECORD: WHERE THE REFERENCE MAN ENTERED THE DIAGNOSTIC MANUAL
What Is Actually Happening Biologically When Gender Bias in Medicine Produces Diagnostic Failure?
In 1977, the United States Food and Drug Administration issued guidance formally excluding women of childbearing potential from early-stage clinical trials. We reference this a lot - due to the ongoing devastating knock on effects it continues to have for generations of women. The rationale (to exclude women of childbearing potential) centred on "fetal protection", liability management, and the complexity of the menstrual cycle as a research variable — a biological reality so inconvenient to research design that half the human population was removed from the data rather than accommodated within it. The guidance remained in place until 1993. Sixteen years during which foundational research on drug safety, disease presentation, and metabolic tolerance was conducted almost entirely on male subjects, then applied universally to female patients.
The FDA reversed the policy in 1993. The knowledge deficit did not reverse with it.
The diagnostic criteria currently used in clinical practice, the dosing guidelines attached to medications prescribed daily to female patients in Australia's public health system, the NHS in the United Kingdom, and across the United States, were built substantially on research conducted during a period when female biology was classified as a confounding variable. Female presentation of myocardial infarction was historically classified as atypical — a framing that subsequent research has substantially complicated, establishing that while symptom overlap with male presentation is considerable, important differences in associated symptoms were systematically underweighted. A 2016 study in the European Heart Journal found that women presenting with heart attacks were significantly more likely to have their symptoms attributed to a non-cardiac cause than men with equivalent clinical profiles. The textbook was not wrong about the population it studied. It studied the wrong population.
The hormone misdiagnosis problem is structurally related. Conditions where symptoms are cyclical, hormonally modulated, or present differently across demographics are precisely the conditions most vulnerable to a diagnostic framework derived from male-dominated research populations. Women with ADHD are diagnosed an average of five years later than men despite symptom onset at equivalent childhood ages — the diagnostic criteria were built from research concentrated on hyperactive boys, and inattentive presentations in girls were systemically overlooked. The 2024 EurekAlert research confirmed the diagnostic delay gap. Durham University research confirmed the masking dynamic that produces it: autistic women who adapt their behaviour to social expectations become functionally invisible to assessment tools calibrated to a different presentation.
The neurodivergent women diagnosis gap is not a clinical curiosity. Nearly eighty percent of autistic women receive an initial misdiagnosis — most commonly borderline personality disorder, anxiety disorders, or depression — before an accurate assessment is reached. In Australia, average diagnostic delay for ADHD in women sits at approximately five years beyond the male average. In the United Kingdom, NHS waiting lists for adult autism assessment have extended, in some regions, beyond three years. The women navigating those delays are not presenting unusually. They are presenting through a system that was not built to recognise them.
The medical gaslighting statistics that emerge from patient experience research are not anecdotal. A 2024 study published in the Proceedings of the National Academy of Sciences, analysing 21,851 emergency department discharge notes across two countries, found that female patients were significantly less likely to receive pain medication than male patients presenting with identical complaints — a disparity that held across both male and female physicians. Women waited an average of thirty minutes longer in emergency departments. Their pain scores were ten percent less likely to be recorded by triage nurses. These are not individual clinician failures. They are the measurable output of a system whose research architecture was built around a body that was not theirs.
THE SYSTEM RECORD: WHY THE CORRECTION HAS NOT KEPT PACE
The architecture described across this report was not built through deliberate exclusion. That distinction matters — not because it softens the outcome, but because misidentifying the mechanism tends to produce the wrong corrective response.
The Reference Man was institutionalised because the people who needed a physiological baseline reached for the population they had data on, the population their infrastructure was built to accommodate. In that sense, he was less a cause than a crystallisation — a formal expression of assumptions that already existed across research, industry, and regulatory design. Each individual decision made a certain kind of institutional sense. The accumulation of those decisions produced a built environment calibrated to one body and a medical system with a systematic blind spot operating most powerfully at the intersection of hormonal complexity, chronic condition management, and conditions that were simply not studied adequately when foundational knowledge was being established, which is to say, it operates most powerfully precisely where women's healthcare tends to be concentrated.
The women's health research gap has a financial dimension as well as a scientific one. Analysis by the McKinsey Health Institute and World Economic Forum found that conditions including endometriosis, PMDD, menopause, and maternal health constitute fourteen percent of the total global disease burden as measured in Disability-Adjusted Life Years. Between 2019 and 2023, those conditions received less than one percent of cumulative medical research funding allocated to the sixty-four conditions driving the majority of the women's health gap. The research infrastructure reflects the same hierarchy of attention that produced the Reference Man.
The metabolic rate tables governing thermal comfort in commercial buildings globally still do not adequately account for sex differences. The drug dosing guidelines built from male-dominated trials remain in clinical use. The first biomechanically representative female crash test dummy is three years old. ASHRAE updated its documentation in 2023 without recalibrating the underlying mathematics.
The benchmark is fifty years old. The evidence of its inadequacy has accumulated for a decade. The woman in the Melbourne waiting room with her handwritten list is not a symbol of anything. She is a patient navigating a system built on a baseline that does not include her, in a country with universal healthcare, in 2026. The gap between what is known and what has been corrected is the actual subject of this investigation. That gap has a name too. It just hasn't been standardised yet.
Stay sane out there jungle watchers. Stay informed and we'll help you.
// Georgie / Aubrey Out. //
Report filed by:
Special Agent Georgie Foxglove // BluntBirds Intelligence Division
Special Agent Aubrey Rouge // BluntBirds Intelligence Division
// TRANSMISSION ENDS
*All claims in this report are sourced from peer-reviewed research, verified institutional data, and documented public record. Full source citations are available in the EVElibrium Vault.



Comments